Qu'arrive-t-il aux médecins qui osent sortir des sentiers battus ?
Traduction automatique ici : https://tinyurl.com/uw9pht3a
What Happens to Doctors Who Innovate?
- September 09, 2023 Download PDF
Story at-a-glance
- The medical community has a longstanding bias against acknowledging new evidence which shows existing practices harm patients, and doctors who present it often experience professional repercussions for doing so
- The final part of a doctor’s training is done so they can earn a board certification. That certification is often necessary for doctors to perform things specific to their specialty (e.g., surgeries)
- ABIM is a private “nonprofit” organization that grants most of the board certifications hospitals require a doctor to hold in order to see patients within them. Longstanding concerns exist that ABIM has abused its monopoly to milk as much money as it can from America’s doctors (which is then spent on “executive compensation”)
- During COVID, ABIM chose to revoke the board certifications of numerous doctors who saved lives by publishing effective treatment protocols for COVID-19 no one could make money off of. ABIM’s conduct illustrates how the modern medical system suppresses anything which competes with its business
I chose “The Forgotten Side of Medicine” as the name for my publication on Substack because it touches upon the three critical facets of medicine:
- The art of medicine and depth of doctor-patient relationship — both which are becoming lost as we switch to an increasingly technological and algorithmic practice of medicine.
- The forgotten victims of medicine who suffered much of what the current generation is now also experiencing at the hands of a greedy industry which values profits over human beings.
- Forgotten medical innovations that got lost to history because they challenged the current medical orthodoxy or threatened the medical monopoly.
I recently completed an article discussing how grant system (which only funds orthodox research) has played a pivotal role in causing innovation to disappear from medicine. When I reviewed Pierre Kory’s pending de-certification by the American Board of Internal Medicine (ABIM), I realized those events illustrate another common way critical innovations are prevented from ever seeing the light of day.
Teach More, Get Less
Almost all of my time in the educational system has followed the same pattern. Information gets thrown at students, like spaghetti being thrown against a wall again and again, in the hope some of it will eventually stick.
In my own case, since I tried to learn and understand the information when it first was presented, I “got it” and had the surreal experience of seeing what I was taught in eighth grade be thrown at the wall again and again well into my undergraduate degree. Presently, I believe education should do some combination of the following:
- Force students to learn the foundational material everything else is based upon and drill that into students until it becomes an unconscious competency (e.g., I was fortunate to have this done for me with arithmetic in 3rd grade by a teacher people complained was “too strict,” whereas the majority of adults I meet still struggle with many of the concepts I learned then).
- Find ways to make the concepts understandable, relatable, and interesting so that students who do not do this innately have a bridge to self-learning the concepts.
- Encourage students to critically examine the concepts so they can decide if they agree with the material, be motivated to further explore what they are curious or unsure about and in the process teach themselves to think critically.
Since none of this is prioritized by the modern educational system, we have more and more years of schooling added on that give less and less. For example, a good case can be made that current college students know less (and are tested to a less rigorous standard) than 8th graders were a century ago.
In many ways, the purpose of the educational system now seems to be primarily to support the educational industry, socially condition students who are in it (e.g., by keeping them out of a broader society which would challenge their beliefs), and make everyone be invested in becoming a lifelong cog in the system.
To overcome the understandable resistance many would have to spending years of their life (and tons of money) in learning something of questionable value, a carrot and stick model is used — students are constantly kept under significant pressure to succeed academically so they can make it through each successive hoop and end up where they “need” to be in society.
Specializing in Medicine
Most people would agree that the most elusive carrot dangled before students in the educational system is the chance to become a doctor if they do everything right and work for years and years to be at the top of their class. As a result, many students who go into medicine quite literally spend years of their lives doing nothing but trying to be able to get into medical school.
However, once they get there, something needs to be done to continue to motivate them to give everything they have to continue being trained. The carrot then becomes not simply getting to be a doctor (which is no longer a big deal once they make it medical school) but rather making it into their preferred speciality.
In essence each specialty’s “merit” comes from how much it pays, how many years of training it takes to complete (e.g., family medicine [general practice] takes three years, while neurosurgery takes seven), and how hard the lifestyle is for the specialty (e.g., do you have to work long hours with high risk surgeries and have to sleep at the hospital in case emergencies come in).
Typically, the harder a specialty is, the more it pays. When there is a more favorable ratio between a speciality’s difficulty and salary it becomes more desirable. For example, dermatology only requires completing a four year residency and has a very laid back lifestyle, but pays as much as far more difficult specialities.

Because of this, students go to extreme lengths to get into dermatology and do everything they possibly can to chase the carrots that are given to them throughout medical school.
Likewise, many of other the desired specialities (e.g., cardiology) require completing a fellowship after residency and hence motivate trainees who already made it to their desired residency to continue doing everything they can to chase the carrots presented to them.
Whenever I give students advice on what specialty to go into, my advice is always the same: “you will make more money than you’ll ever need regardless of your speciality — pick the one you actually enjoy rather than the ‘better’ one that burns you out.” Unfortunately, most of them never follow my advice.
As a result, many of classmates have reached their wits ends with medicine and often share how they are wondering when they can afford to retire, whereas I love what I do, I plan to practice until the end of my life, and I even have the bandwidth to take on the immense side-project of writing millions of words online to help set things right with COVID-19.
Note: A close friend who is one of the smartest people I know chose to be a dermatologist. I felt my friend had an immense degree of talent and could have created numerous medical breakthroughs, but instead they chose to go into dermatology so they could be make a lot of money, support their family and not have to work too hard. I share this because this is one of the many ways those who could innovate are incentivized not too.
If you take a step back and look at all the specialization within medicine, an interesting phenomenon emerges — doctors keep on needing to train for more and more years, but it’s hard to say how much there is to show for it. A century ago, medical graduates entered practice after completing four years of medical school.
Then internships (a year of hospital training after graduating medical schools) got gradually phased in. After that, medical residencies gradually got phased in, and finally fellowships got phased in (and in some cases multiple fellowships).
Yet, the benefits of this proliferation of medical education are somewhat questionable — for example doctors during COVID-19 demonstrated less ingenuity and ability to adapt to the needs of their patients than doctors did a century ago during the 1918 influenza. Likewise, many of us (e.g., Pierre Kory) have noticed that the specialists are less able to help patients than general practitioners and typically all just say the exact same thing — especially within a hospital setting.

Download this Article Before it Disappears
Download PDFBoard Certification
Since most states only require completing one year of residency to practice medicine (although this is starting to change at the state level), something needs to be done to ensure the carrot to pursue a medical residency can still be dangled in front of doctors long after they graduate medical school.
This is done by tying a lot of privileges to being board certified, and having it (for the most part) only be possible to become board certified if you complete a residency or post-residency fellowship. Some of those privileges include:
- Being able to see patients in a hospital (board certifications are typically required for hospital privileges).
- Being able to receive insurance reimbursements for the procedures your speciality has monopolized (e.g., the high paying ones a lucrative specialty has monopolized).
- Being less likely to lose a malpractice case and hence having lower malpractice insurance.
- The social status a board certification provides (e.g., being a “cardiologist”).
Nonetheless, many eventually opt to relinquish their board certifications because they realize they hate working within the conventional medical system and maintaining the certification is expensive and a lot of pointless hassle.
De Facto Laws
One of the important but under appreciated distinctions in law are “de facto laws,” things that were never formally made into law but are nonetheless treated as law. De facto laws essentially make it possible for people to bypass the legal process (which is meant to protect the public from tyranny) but nonetheless still have the force of the law behind them.
For example, as we all saw during COVID-19, a coordinated effort was made to censor any information which suggested treatments (that no one could make any money off of) existed for SARS-CoV-2, and to outlaw the administration of drugs that could treat it. This was all illegal, but since everyone (e.g., law enforcement, hospitals and insurance companies) deferred to the authorities advocating those positions, they became law.
Likewise, there has been a longstanding issue where corrupt panels are appointed to provide guidelines for treating diseases which always end up supporting the interests of the sponsors of those panels. This was best illustrated by the NIH panel that officially decided what treatments were appropriate to treat COVID-19 in the hospital which then became a de-facto law.
In the case of that panel, its members were directly appointed by Fauci (who was heavily invested in remdesivir), most of them had significant financial ties to remdesivir’s manufacturer, and not surprisingly, despite a lot of against remdesivir, they voted for their drug to be the standard of care for COVID-19, a decision that cost thousands of American lives.
Sadly, this is not by any means an isolated case and there are many other cases of corrupt panels pushing unjustifiable guidelines into medical practice (e.g., consider the recent decision to add the COVID-19 vaccine to childhood vaccine schedule despite children having a real risk of a vaccine injury but no risk of COVID-19).
Likewise, prior to COVID-19, one of the most impactful examples was paid-off panel that decided everyone needed to be on statins even though an independent group using the same set of studies reached the opposite conclusion.
One of the most important things about these de facto laws came from a 2017 lawsuit filed by Lyme patients against the Infectious Diseases Society of America (IDSA), an authoritative group which publishes guidelines I frequently don’t agree with (e.g., they argued for remdesivir to treat COVID-19) The lawsuit was ultimately dismissed by a judge because:
“IDSA’s guidelines [for Lyme disease] … make clear that adherence to the guidelines is voluntary, with the ultimate determination regarding their application to be made by the physician in light of each patient’s individual circumstances.”
I feel this ruling is noteworthy because IDSA’s guidelines were a de-facto law for Lyme patients but the judge allowed the IDSA to argue they were not and hence have the lawsuit dismissed.
This for context was the exact same argument the FDA used to dismiss the lawsuits against it for illegally suppressing ivermectin (the FDA claimed it never prohibited the use of drugs like ivermectin; rather it simply gave suggestions people could chose to follow or to not follow that were not legally binding).
Since the IDSA ruling has not been challenged, it is the current precedent which should guide these types of cases and may explain why the FDA recently reversed its position:
“FDA explicitly recognizes that doctors do have the authority to prescribe ivermectin to treat COVID,” Ashley Cheung Honold, a Department of Justice lawyer representing the FDA, said during oral arguments on Aug. 8 in the U.S. Court of Appeals for the 5th Circuit.
Note: They may have also reversed their position because COVID-19 is over, so there is no longer a financial incentive to suppress treatments that compete with commercial interests.
Try to keep the premise that that guidelines should not constitute de facto laws in mind as we look at the ABIM’s justification for targeting physicians with dissenting opinions.
Speciality Boards
In order for doctors to practice medicine, they need to have a medical license, which requires completing medical school, passing some exams, and successfully completing at least one year of a medical residency within the United States. Doctors are always in fear of losing their medical license (as there are a lot of technicalities a medical board can chose to target a doctor’s license with).
In turn, the threat of industry sponsored medical boards has been one of the main things that has kept doctors from ever going too far out of the box (e.g., very few physicians I know will do integrative cancer treatments for this reason — and those that do so do as discretely as possible).
However, while there are serious issues with the medical boards, their conduct varies state by state (e.g., only the highly liberal states went after doctors who dissented from the COVID narrative — leading to many doctors relocating to red states so they could still practice medicine) and there are certain laws they are all required to follow.
The speciality boards, by virtue of being private entities that were never inshrined by a law they are accountable to have much more latitude to do whatever they want. Since most doctors need a board certification from a specialty board to practice, this allows speciality boards to make a variety of de-facto laws.
Prior to COVID-19, most of these laws were primarily motivated by greed — the specialty boards kept on charging doctors more and more to maintain their board certifications and then keeping the money for themselves.
In response to this, many physicians have left their board certifications go. Conversely, others have begun to file more and more lawsuits against the speciality boards (and other related groups feeding off the same trough) for this monopolistic exploitation.
One of the more egregious offenders has been the American Board of Internal Medicine (ABIM) the group responsible for certifying each doctor who works in the hospital and the various organ specialists (e.g., cardiologists). To quote Pierre Kory:
“I think that I had to pay upwards of $1,800 for my last Board re-certification [along with all the time needed to prepare for it]. And get this - that money essentially goes to ABIM executive salaries and pensions and other dubious private investments as described by Eichenwald where he details the insane lengths the ABIM goes to "hide” the compensation and pension data on its executives.”
As hard as this is to believe, Kory’s description underplays the ABIM’s malfeasance. Eichenwald’s investigation for Newsweek in 2015 found:
- ABIM executives were receiving between 1-2 million dollars in annual salaries (which should be in the 100k-200k range).
- That the ABIM, a nonprofit, was doing everything it could to hide that compensation.
- That ABIM was aggressively pushing physicians to do onerous and completely pointless things to maintain their board certifications so they could milk more money from them.
- That the ABIM was engaging in anti-competitive practices against anyone who tried to create an alternative to their model.
In short, the investigation called for Congress to investigate ABIM and break up its monopoly because of how many physicians were adversely affected by its greed.
As you might have guessed, ABIM was one of the more inclined parties to push for the pharmaceutical narrative. So once doctors began dissenting against the COVID-19 narrative, ABIM moved to revoke their board certifications (e.g., this was done to Peter McCullough, Paul Marik and Pierre Kory last June).
This was an interesting move on ABIM’s part because the doctors it targeted were highly respected leaders in their field (e.g., Paul Marik is considered by many to be the leading author in the field of critical care [ICU] medicine), so if anything, the targeted doctors should have been the experts the specialty deferred to rather than the ones it kicked out.
Some of the doctors eventually decided to fight back (e.g., AAPS sued the speciality boards last year). Pierre Kory likewise has tried to work through ABIM’s onerous and futile appeal process. When I asked him what was motivating him and Marik to go through the grueling process to challenge their decertification (e.g., producing a 60 page response), he told me:
“I’m done with these people. I don’t need the board certification because I never want to work in a hospital again. However, on principle I need to fight this because a lot of other doctor do and they are trying to make an example out of us so all those doctors stay in line and comply.”
Additionally, Kory also shared an important point Meryl Nass had pointed out:
“Suddenly claiming that using licensed drugs for COVID, criticizing federal policies for COVID or criticizing the value of COVID vaccines is “unprofessional” gives the specialty board the right to revoke a certification — well, that was never part of its contract with me.
So pulling my certification for issues that were never specified in the original contract is breach of contract. Well, that is if contracts, like constitutional amendments and medical ethical principles were still “a thing.””
Given how much work doctors make to become board certified (and then maintain the certification), what Nass highlights is a serious infraction on the ABIM’s end. This is something I believe all physicians, including those who completely support the COVID-19 narrative should oppose, as it is simply another facet of how doctors in this country have all been increasingly exploited by the specialty boards.
ABIM’s Charges
Since the ABIM is a private group that can make de facto laws as they please, to some extent, the reasons they chose to go after the COVID dissidents are ultimately arbitrary. Nonetheless, I think there is still quite a bit to be learned from their allegations (which can viewed here).
The crux of their argument is that alternative treatment protocols authored for COVID-19 (e.g., the use of ivermectin) were harmful misinformation and thus justified a revoking board certifications.
This reasoning is interesting, because as far as I know, while I’ve frequently seen cases of a doctor losing their state medical license for conduct that endangers the public, I’ve never seen a physician have a board certification be revoked as a punishment (even in cases where the physician was caught being a serial sexual predator or doing countless unnecessary surgeries that severely injured or killed numerous patients).
Rather, a board revocation typically only happens when a doctor didn’t give the speciality board all the money it wanted. One of the passages in the ABIM’s letter is particularly illuminating:
“[ABIM] concluded that your statements about the purported dangers of, or lack of justification for, COVID-19 vaccines are false and inaccurate because they, too, are not supported by factual, scientifically grounded, and consensus driven scientific evidence.
In fact, the overwhelming body of factual, scientifically grounded, and consensus-driven evidence – at and since the time you made those statements – shows that the COVID-19 vaccines are safe and effective for children and for adults.”
Kory and Marik submitted a litany of evidence to support their protocols. All of that evidence was ridiculed and ignored, with the ABIM instead cited a few questionable studies to support its position and then argued it was right because its position was “the consensus.” After seeing the ABIM’s rationale for their conduct, a few issues jumped out at me.
First, some of the information (discussed below) the ABIM cited to defend their position appears to be misinformation. This creates a catch-22, since by the standards ABIM is putting forward, the physicians in ABIM leveling these charges against others need to be dismissed by the ABIM for conveying misinformation and thus should not be able to present those charges in the first place.
Second, the consensus with COVID-19 has changed multiple times, and the ABIM’s position will likely be viewed as erroneous by the mainstream medical community within a few years as there is already significant scientific evidence challenging it. Since that evidence already exists, once public opinion shifts and it becomes the consensus, ABIM’s decision to provide a willful dismissal of this evidence (in writing) will likely become a huge issue for the organization.
Third, consensus based medicine is not the same as evidence based medicine.
Evidence-Based Medicine
When I first entered the medical profession, a mentor told me that the medical field was remarkably stubborn and frequently resisted changing bad ideas for decades.
In the 1980s, the need to overturn entrenched dogmas with scientific evidence began to gain traction, and in 1990, Gordon Guyatt coined the term “evidence based medicine,” (EBM). Then in 1996, David L Sackett, published a widely cited article defining exactly what EBM was:
“The conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.”
Put differently, Sackett, proposed that three different considerations needed to be weighted equally in evidence based clinical practice:
- Patient Values
- Clinical Expertise
- Relevant Research
So if for example, a patient did not want to be vaccinated, it would not be evidence based practice to pressure them to vaccinate and deny them care them if they did not vaccinate (something that as whistleblowers have testified happened throughout the pandemic).
Likewise, if a doctor’s clinical experience told them one therapy that was not supported by the guidelines was the safest and most effective therapy for a patient, the doctor would not have to risk their medical career being destroyed or having to sue their hospital to administer it (both of which happened to Paul Marik).
Note: As detailed in The War on Ivermectin, there were 80 lawsuits where families with a relative being subjected to Fauci’s hospital COVID protocols and was expected to die had lawyer Ralph Lorigo sue the hospital for ivermectin to be administered to their relative.
Of those 80 lawsuits, in 40 the judge sided with the family, and in 40 with the hospital (initially the lawsuits were successful, but as they mounted, the hospitals banded together to develop an effective apparatus to dismiss further lawsuits).
Of the 40 cases where ivermectin was given, 38 of the 40 patients survived. Of the 40 cases where the hospitals were allowed to withhold ivermectin, 2 of the 40 patients survived. Beyond the fact this is insane, like the vaccine mandates, it is also a perfect example of not following the three pillars of EBM.
Since Sackett’s 1996 article had such a large influence on the practice of medicine, I think it is helpful to cite of it:
“Increased expertise is reflected in many ways, but especially in more effective and efficient diagnosis and in the more thoughtful identification and compassionate use of individual patients' predicaments, rights, and preferences in making clinical decisions about their care.
Good doctors use both individual clinical expertise and the best available external evidence, and neither alone is enough. Without clinical expertise, practice risks becoming tyrannised by evidence, for even excellent external evidence may be inapplicable to or inappropriate for an individual patient. Without current best evidence, practice risks becoming rapidly out of date, to the detriment of patients.
Evidence based medicine is neither old hat nor impossible to practice. The argument that "everyone already is doing it" falls before evidence of striking variations in both the integration of patient values into our clinical behaviour and in the rates with which clinicians provide interventions to their patients.
The argument that evidence based medicine can be conducted only from ivory towers and armchairs is refuted by audits from the front lines of clinical care where at least some inpatient clinical teams in general medicine, psychiatry, and surgery have provided evidence based care to the vast majority of their patients.
Evidence based medicine is not "cookbook" medicine. Because it requires a bottom up approach that integrates the best external evidence with individual clinical expertise and patients' choice, it cannot result in slavish, cookbook approaches to individual patient care.
External clinical evidence can inform, but can never replace, individual clinical expertise, and it is this expertise that decides whether the external evidence applies to the individual patient at all and, if so, how it should be integrated into a clinical decision.
Similarly, any external guideline must be integrated with individual clinical expertise in deciding whether and how it matches the patient's clinical state, predicament, and preferences, and thus whether it should be applied. Clinicians who fear top down cookbooks will find the advocates of evidence based medicine joining them at the barricades.
Some fear that evidence based medicine will be hijacked by purchasers and managers to cut the costs of health care. This would not only be a misuse of evidence based medicine but suggests a fundamental misunderstanding of its financial consequences.
Doctors practising evidence based medicine will identify and apply the most efficacious interventions to maximise the quality and quantity of life for individual patients; this may raise rather than lower the cost of their care. Evidence based medicine is not restricted to randomised trials and meta-analyses. It involves tracking down the best external evidence with which to answer our clinical questions.
Because the randomised trial, and especially the systematic review of several randomised trials, is so much more likely to inform us and so much less likely to mislead us, it has become the "gold standard" for judging whether a treatment does more good than harm. However, some questions about therapy do not require randomised trials (successful interventions for otherwise fatal conditions) or cannot wait for the trials to be conducted.”
I would thus argue that the response to COVID-19 was not evidence-based medicine.
Consensus Based Medicine
Throughout COVID-19 we saw consensus-based medicine (CBM) masquerading as evidence-based medicine be forced upon America and had our eyes opened to exactly why EBM is so important the practice of medicine.
CBM is why doctors were not allowed to utilize protocols they saw were keeping their patients alive and instead were forced to use protocols created by corrupt committees that killed thousands of Americans and created the urgent need for a vaccine to end the pandemic.
Likewise, CBM was why an unproven, dangerous, and ineffective vaccine was allowed to remain on the market, why every doctor who challenged it was cancelled, and why the response to all these concerns was instead to mandate the vaccine and gaslight everyone who was injured by it.
Since you are already familiar with many of the examples, I would like to cite one that was raised by ABIM to Dr. Kory:
Every drug is toxic (hence why I use them sparingly), and while ivermectin is not 100% safe (reversible symptoms will occur in sensitive patients), it is one of the safest drugs in existence. For example, I do not know of any documented cases where someone has died from an ivermectin overdose (I only know of three “suspected” cases where more information was not provided). This is a distinction very few other drugs hold as virtually any drug can be deadly at a high dose.
Since ivermectin (a Nobel Prize winning drug) threatened the money the pandemic profiteers were going to make from COVID-19, it needed to be rebranded as deadly and ineffective. One of the initial strategies employed for this was to create a barrage of sensational media reports like this one:
What was so amazing about this story was that despite its patent absurdity (e.g., all of it was fake — including the above picture), it was nonetheless taken up by media outlets around the world, and to this day most people are still unaware it was made up. The NPR article cited by the ABIM cited made a few important points:
First, it restated Rolling Stone’s position that ivermectin overdoses were flooding ERs.
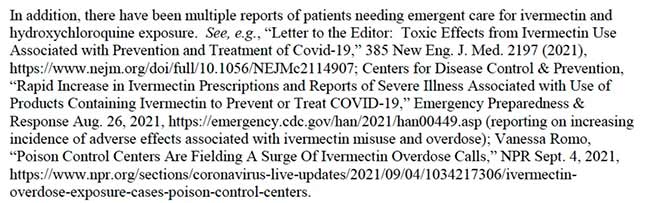
Second, without stating it explicitly, it acknowledged that all of the extra cases of ivermectin overdoses came from people incorrectly self-medicating with the veterinary formulation (the paste) since there was a 70% increase in overdoses and 70% of the overdoses were thought to have come from the paste. This is important because that is entirely different from the precise dose of the pills made for humans Kory and others advocated for appropriately prescribing to patients.
Third, the source the NPR article cited indicated that for the first 8 months of 2021, compared to 2020 or 2019, of the approximately 728 extra cases, 0 died, 1% (roughly 7) had a “major” effect, 8% had a “moderate” effect (roughly 58), 13% (roughly 95) had a “minor” effect, 20% had no effect, and of the 58% not followed, the majority were not thought to have had a significant effect from the ivermectin.
What this means is that there was an understandable increase in calls to poison control centers by people who had decided to take veterinary ivermectin and then became were worried they’d misdosed it. Nonetheless, nothing of consequence happened (seven people in the entire country had “major” reactions).
Conversely, there are slightly over 2 million calls to poison control each year, 567,035 of which come from just seven types of pharmaceutical drugs. One category (responsible for 136,380 calls), “analgesics” is predominantly comprised of the same drugs (e.g., ibuprofen or Tylenol) that doctors around the country (along with healthcare authorities and the media) told patients take if they came down with COVID-19 to pass the time until they needed to be hospitalized and possibly die.
Note: In addition to their inherent dangers, I and colleagues consistently saw fever-suppressing analgesics worsen the course of COVID-19 infections and France went so far as issue a formal warning against using ibuprofen for the disease.
Compared to ivermectin “poisonings” (which have resulted in 0 deaths), each year in America, preparations of Tylenol intended for human use result in 26,000 hospitalizations, 56,000 emergency department visits and 500 deaths annually. As you all know, no one was ever punished for telling patients to self-medicate with these drugs.
I share this example to illustrate why consensus based medicine is so problematic. If evidence based medicine was followed, none of this would have ever happened.
Historical Examples
Medicine’s history is marked by bad medical practice after bad medical practice being medical dogma for decades if not centuries. In turn, there are countless cases of a physician challenging the bad medical practice being viscously attacked by their peers for years and often only acknowledged long after their death.
Since this is the “culture” of medicine it has allowed things like the current disastrous medical practice — mandating a deadly and ineffective vaccine for an extinct virus (the strain the vaccine “protects” against no longer exists) upon the population — to be accepted and largely unchallenged.
Since history is often extremely instructive for understanding where we are now, I’d like to review some of the previous medical dogmas my profession did everything it could to hold onto:
• Not washing hands after dissecting corpses and then delivering babies. The doctor who pointed out this was killing thousands of mothers grievously offended his peers, was attacked by them, and was eventually committed to a mental asylum where he suffered a fatal beating.
• Frontal lobotomies for mental illness became such a common medical practice they won the inventor a Nobel Prize.
• Long ago, a cardiologist I knew who believed it was necessary to give anticoagulants for heart attacks was relentlessly attacked by his peers for endangering his patients and suffered severe professional consequences. His approach is now the standard of care in cardiology.
• Long ago, there was a belief that anyone who survived a heart attack needed 4-6 weeks of complete bed rest enforced by the hospital so their heart would not be stressed. This was torturous for the patients and appeared to make them much more likely to develop severe complications or die. A cardiologist who felt terrible for what these people were going through eventually decided to test this approach:
“Little did I realize that violating firmly held traditions can raise a tsunami of opposition. The idea of moving critically ill patients into a chair was regarded as off‑the‑wall. Initially the house staff refused to cooperate and strenuously resisted getting patients out of bed.
They accused me of planning to commit crimes not unlike those of the heinous Nazi experimentations in concentration camps. Arriving on the medical ward one morning I was greeted by interns and residents lined up with hands stretched out in a Nazi salute and a “Heil Hitler!” shouted in unison.”
The experiment was a success and dramatically reduced the death rate (to a third of what it had been), making it still be the most successful measure in history for reducing the death from heart attacks.
Dr. Malcolm Kendrick did the math and concluded that the old approach was responsible for more deaths the first and second world wars, Stalin’s pogroms, and the Holocaust, added together. Once the dust settles, I can only imagine how the COVID-19 guidelines will compare to that down the road.
Note: There are countless other examples of a disastrous consensus being medical dogma that similarly resisted all attempts to overturn it. For length considerations, I avoided listing 25 other notorious examples compiled by the FLCCC which can be viewed here.
Conclusion
I believe the ABIM’s conduct is extremely short sighted — both for the organization since it shines a bright light on their unscrupulous business practices that no practicing physician supports and for the medical industry in general.
One of the major fears a significant segment of the public has now is if it’s safe to go to hospitals because they understandably believe the hospital and the doctors there will prioritize what makes the hospital money over what keeps the patient alive.
The fact that many patients chose to sue their hospital to get what they believed to be a lifesaving treatment be administered (or bypassed the hospital entirely and secretly administered it) indicates much of the trust my profession spent decades building has been lost.
Everyone loses from this — the hospitals have less visits and hence take in less money, the doctors have much more difficult interactions with their patients, and patients who need hospital care avoid it. An important point to emphasize is that while I disagree with some standard hospital practices (e.g., beyond COVID, its unforgivable vitamin C is almost never given to septic patients) many others are excellent and consistently lifesaving.
Likewise, I’ve known famous natural medicine advocates who were deathly afraid of being murdered at a hospital that refused to seek hospital care for a very easy to treat condition and died as a result of that decision.
Making examples out of the public figures Americans would most want to be their hospital doctor is the exact opposite of what the medical industry should be wanting to do right now — especially when it is done by the group that determines if doctors can work in hospitals. Recently, a national survey conducted since 1972 found the same thing:
- Only 39% of Americans (and 22% of Republicans) now have “a great deal of confidence” in the scientific community (down from 48% collectively in 2018).
- 13% of Americans have “hardly any” confidence in the scientific community now.
- Only 34% of Americans (and 26% of Republicans) now have a “great deal of confidence” in medicine (down from 39% in 2018).
I believe if we allowed doctors who had the best intentions of their patients to innovate, the public would have much more confidence in the medical profession.
A Note From Dr. Mercola About the Author
A Midwestern Doctor (AMD) is a board-certified physician in the Midwest and a longtime reader of Mercola.com. I appreciate his exceptional insight on a wide range of topics and I'm grateful to share them. I also respect his desire to remain anonymous as he is still on the front lines treating patients. To find more of AMD's work, be sure to check out The Forgotten Side of Medicine on Substack.



Commentaires
Enregistrer un commentaire