Déterminer les risques et les avantages de chaque vaccin recommandé.
De : https://www.midwesterndoctor.com/p/determining-the-risks-and-benefits?
Traduction automatique ici : https://tinyurl.com/yw4ff5ts
How to Navigate Which Vaccines To Give Your Children


Story at a Glance:
•The
blatant dishonesty of our drug regulators throughout COVID-19 has led
to many realizing they can’t trust that other recommended vaccines are
“safe,” “effective” and “necessary.”
•Since many people have asked me about this topic, I’ve worked to produce an independent assessment of each recommended vaccine.
•This
is a surprisingly challenging calculation to make which is extremely
prone to the assessor’s bias, and remarkably, in many cases, the data we
need to determine the risk and benefits of each vaccine accurately does
not exist.
•In this article, I attempted to provide the best assessment I could of each CDC recommended vaccine. In some cases, it is very clear the risks outweigh the benefits of a vaccine, while in other cases, it is less clear. For those on the fence about vaccinating, I believe it is best to initially pay attention to avoiding the worst vaccines.
Note: due to the immense interest in the initial version of this post, I have significantly revised it and added a lot of initial information for those interested in this topic.
One of the common questions I get from readers is “Which vaccines should their kids get?” This is surprisingly difficult to answer because it requires accurately weighing the likelihood of an adverse event from a vaccination vs. the likelihood of suffering a complication from the disease that the vaccine would prevent you from getting, and each of those figures is a fairly complex calculation. If you do however begin to dig into it, you’ll often discover the data necessary to answer this question simply doesn’t exist and instead has been replaced with the blind declaration that each vaccine is “safe and effective.”
This touches upon what I believe is one of the greatest issues our society faces. Most human beings (regardless of their expertise) will selectively filter their perception of reality so that they ultimately only see what conforms to their pre-existing biases. In the case of vaccines, the media trains us to hyper-focus on the rare cases of an unvaccinated individual becoming ill from a disease a vaccine could have prevented while simultaneously ignoring the large numbers of people who develop severe or chronic complications from vaccines.
Fortunately,
COVID-19 provided a once in a lifetime opportunity to actually answer
this question, and in turn, we’ve been able to determine that:
•The COVID-19 vaccine has a significantly greater rate of complications than the disease it prevents.
•The vaccine is only partially effective in preventing COVID-19, and that efficacy rapidly declines with time.
•The large studies of the vaccine show once deployed, it makes things worse not better.
In short, it’s very hard to argue that the benefits of that vaccine outweigh its risks. Remarkably, this has not deterred all the federal health agencies from recommending (or mandating it), even to those who have no risk at all of dying from COVID-19 (e.g., children), irrespective of the public protest they’ve faced. This in turn raises a fairly simple question—does that conduct suggest we can blindly trust their recommendations on the other vaccines (which in almost all cases those agencies rubber stamp and push upon America)?
The Risks and Benefits of Vaccines
From
looking into this question at length, much as is in the case for the
COVID vaccines, I have concluded that for many of the widely used
vaccines:
•Many of the benefits attributed to a
vaccine (e.g., preventing the disease, preventing transmission of it, or
preventing severe complications of it) are much less than the public
(or the medical field) is led to believe.
•Many of the justifications used to justify vaccination are based on historical realities that no longer apply today.
•In cases where a vaccine actually “works” natural selection will quickly make the vaccine stop working.
•Side
effects from vaccination are so frequent and varied that any assessment
of a vaccine’s risks will inevitably miss many of the actual problems
vaccination entails.
In short, I feel a very high bar must be met for vaccination, but as we saw with COVID-19, it often is not.
To accurately determine the risks and benefits of a vaccine, you need to consider all of the following
Disease Risk
If you review the vaccine schedule, very few of the diseases in it have both a significant likelihood that you will get them and a significant likelihood that they will develop into a severe condition. Many of the diseases believed to fall into this category are no longer an issue in the United States (e.g., polio or smallpox). Unfortunately, people who look at this question are often fixated on the past presentations of the disease when it was far more pathogenic or when we did not have a way to treat it. Let’s now look at some of the specific questions one might ask to evaluate this question.
How likely is it for a person to get the disease?
Some diseases we vaccinate against are incredibly rare (e.g., tetanus or polio) while others are now non-existent (e.g., diphtheria).
How likely is the disease to cause a negligible, minor, moderate, severe, or fatal complication?
It is very important to distinguish between these categories because, for most infections, the risk of catching it and then subsequently getting a severe case of the condition is extremely low. For example, a Neisseria meningitidis infection (which can cause septic meningitis) is really bad and can progress very quickly, but also very rare for people to develop (one in ten people are asymptomatic Neisseria meningitidis carriers whereas approximately one in a million get septic meningitis from it each year).
Likewise,
we vaccinate everyone against chickenpox despite the fact it almost
never causes issues (e.g., only 1 in 100,000 children who get it die
from it, many of whom are individuals with pre-existing immune
suppression).
How likely is it that the severity of the disease can be improved with an existing medical treatment?
Most of the infections we vaccinate against (e.g., pertussis) are very easy to treat. Unfortunately, the focus is always on vaccinating against the disease rather than providing treatment for it (especially if the treatment is something more unorthodox than an antibiotic). In the case of COVID-19, while severe complications represent the minority of cases, they (and the more minor ones) can in most cases easily be prevented by early outpatient treatment. Unfortunately, the Federal government has refused to sanction effective treatments for COVID-19 and instead keeps pushing an endless number of unsafe and ineffective boosters for the disease.
How likely is it that you will have access to the necessary treatment before you get seriously ill?
While I have many criticisms of the vaccine approach, I have to acknowledge that this area is one of the strongest arguments for it. With rapidly progressing diseases, those in isolated areas, those unable to recognize their need to seek medical care, and those of limited economic means, often cannot get the necessary treatment for the disease before it is too late to prevent a severe complication. Hence, if the disease can be “prevented” through mass immunization, it mitigates the unfortunate circumstances that arise when care for a dangerous infection is not immediately available.
Vaccine Efficacy
How likely is the vaccine to be effective in preventing the disease, and does the presence of vaccine antibodies correlate with a decreased risk of the disease?
Many vaccines fail to do one or both of these. COVID-19 has provided the greatest red pill in history on this topic, especially since successive COVID-19 vaccines, despite increasing antibody levels, actually increase your risk of catching the disease.
How likely is the vaccine to be effective at preventing severe complications of the disease?
The
human papillomavirus vaccine (which “prevents” cervical cancer) is an
excellent example of a vaccine that does not live up to its promise to
do so because its promise was based on a series of assumptions and
wishful thinking.
Note: those assumptions are that
the vaccine will generate antibodies to HPV, that those antibodies will
prevent an HPV infection from forming, that a chronic HPV infection is
the primary cause of cervical cancer and hence that the vaccine will
prevent cervical cancer. Amongst other things, the vaccine actually increased one’s risk of cervical cancer
if one had a pre-existing HPV infection and likewise, population wide
datasets do not contain the expected drop in HPV that had been expected
following the rollout of the vaccine.
How long does the vaccine’s protection last following immunization?
Many
vaccines suffer from declining immunity, hence needing repeated
boosters, which re-expose the recipient to the vaccine's risks. COVID-19
again has provided the greatest red pill in history on this topic, as immunity from it wanes approximately three months
after the most recent injection. Many other vaccines also suffer from
this issue, which must be taken into account when assessing their risk
to benefit ratio.
To illustrate, if something has a
10% chance of injuring you and only protects you for 3 months after
which point it must be taken again, it’s hard to justify taking it,
whereas if something has a 10% chance of injuring you but it protects
you for life, the justification is stronger. Unfortunately, many
vaccines that only provide temporary immunity are marketed in a manner
that implies they provide permanent immunity (e.g., this is what was
initially done with the COVID-19 vaccines).
How likely will it be for the vaccine to prevent you from getting the disease when you need to be protected?
The hepatitis B vaccine is routinely given at birth, and then twice more very early in life. This is nonsensical for two reasons. First, at the time of birth, infants lack an immune system that can mount a proper antibody response to the vaccine. Second, hepatitis B is spread by blood-to-blood contact (e.g., sharing heroin needles or having unprotected sex), both things are very unlikely to happen in early childhood. This is important because the hepatitis B vaccine typically only lasts for around 6-7 years (estimates vary). The best explanation I have seen for why the vaccine is given immediately following birth (despite being completely unjustifiable) is that it habituates parents to come in for regular well-child vaccination visits starting at two months of age.
How long does it take for the vaccine to create a selective pressure that causes the pathogen to no longer be covered by the vaccine?
This is a huge problem for any vaccine that “works” because it rapidly creates selective pressure for variants not covered by the vaccine’s antigen (which is particularly true for encapsulated bacteria). The only vaccines that do not suffer from this issue are the ones where the vaccine does not create selective pressures against the vaccine (e.g., against the non-contagious tetanus bacteria’s toxin) and live attenuated vaccines since they contain so many different antigens.
Note: except for tuberculosis and a few rarely used vaccines, all live attenuated vaccines are viruses. Unfortunately, live attenuated vaccines can cause infections of the vaccine strain in the immunocompromised host and are frequently contaminated with other viruses present in the medium used to cultivate the virus.
For example, Haemophilus influenzae type b (Hib), an encapsulated bacteria, was one of the most common causes of bacterial meningitis, and prior to a vaccine for it existing, per the CDC, 20,000 young children got a severe case of Hib and 1,000 died, whereas now (after the vaccine came out in 1985-1987), less than 50 children get a severe case of Hib disease. This is an extraordinary change, and many of my colleagues who were in practice when the vaccine came out hence support it because they immediately saw the difference in meningitis cases at their hospital which are very sad.
Because the vaccine worked, it created selective pressure for Hib to resist the vaccine resulting in non-typable strains of Haemophilus influenzae becoming much more common. Some of those strains are quite dangerous and as this study shows, they hospitalize and kill children, and unlike Hib, also affect older adults (resulting in adults who never previously had to worry about Haemophilus influenzae infections developing meningitis from it).
Because this is a longstanding problem, many theorized that the COVID-19 vaccine (due to it only containing a single antigen in a rapidly mutating part of the spike protein) would rapidly trigger the production of pathogenic variants. This is, of course, what happened soon after it hit the market. Likewise, the pneumococcal vaccine (which is another encapsulated bacteria), is widely given to both children and adults (e.g., to prevent pneumonia) creating selective pressure for bacteria to no longer be covered by the vaccine. Because of this, as the years go by, antigens from more and more pneumococcal variants (strains) need to be added to the vaccine (e.g., originally it had 7, but now it has 23).
Does the vaccine provide immunity from the disease or its symptoms?
In many cases (e.g., with pertussis or COVID-19), the immune response generated protects you from an effect of the disease (e.g., the pertussis toxin) rather than catching the disease itself. Because of this, outbreaks are frequently observed in vaccinated populations (e.g., consider how often this happened with COVID-19 despite us repeatedly being promised the vaccines would end the pandemic).
Can the vaccine be taken therapeutically?
Typically with a vaccine, you have to balance the theoretical risk of it preventing a dangerous infection against the guaranteed risk of it causing harm. However, in some cases, a vaccine can be taken after an infection develops, making it a therapeutic rather than a preventative vaccine (e.g., one way the COVID vaccines were marketed was as a treatment for Long COVID despite the fact this was never proven and vaccination often making Long COVID much worse).
For
example, rabies is a slowly progressing but highly lethal disease.
Because of this, if one is vaccinated after a rabies bite, a rabies
vaccine will often save their life (whereas there are very few other
therapeutic options for these situations). As a result, many argue a
therapeutically administered rabies vaccine is one of the most
justifiable arguments for vaccination.
Note: the rabies
vaccine is one of the more dangerous vaccines, so it is much harder to
argue for its use as a preventative (e.g., for people who will regularly
work with animals). Likewise, I’ve seen numerous cases of someone
receiving the vaccine after being bitten by an animal where it was not
known if the animal was rabid or it was later discovered the animal
wasn’t rabid and in those cases, I know of numerous people who seriously
regret their choice to get the rabies vaccine (due to the complications
they experienced).
Likewise, I have seen many cases of recurrent shingles being treated by the shingles vaccine. While this is not my preferred approach (since it has risks), I know many people who avoided its side effects and are immensely grateful that the vaccine protected them.
Does the vaccine have other benefits besides preventing the disease?
Some
live attenuated vaccines broadly stimulate the immune system. In
third-world countries with a high infectious disease burden, this
actually saves lives (this has been shown
with the measles-mumps-rubella vaccine [MMR] and the tuberculosis
vaccine [BCG]) because the immune system is better able to fight off
otherwise fatal infections for which modern medical care is not
available.
Note: conversely, other vaccines like DPT, when studied were found to do the opposite and broadly increase the risk of death due to the immune suppression they create.
Likewise, therapeutic effects are occasionally found for specific vaccines. For example, the BcG vaccine has been shown to treat certain types of bladder cancer and is now a mainstay of treatment.
Population Immunity
Assuming that the vaccine “works”:
Does vaccination creating a selective pressure for vaccine resistant variants to produce more or less dangerous variants?
With
certain vaccines, the strains created by the selective pressure of the
vaccine are more dangerous than those that preceded them, and they
affect different age groups. As discussed in the previous section, this
has occurred with the pneumococcal and Hib bacteria along with the
COVID-19 virus. Additionally, it has also occurred with other
infections (e.g., HPV and pertussis).
In some cases this has been a problem. For instance, as mentioned before, now haemophilus influenzae affects older adults, while the COVID-19 vaccine caused a variety of harmful variants to become the circulating strains. Likewise, in the case of pertussis, the new variants it created have a variety of issues such as one releasing more of the pertussis toxin and having a higher rate of hospitalization and deaths and them affecting older age groups.
Note: this shift to older adults was also seen with the Hib vaccine and pneumococcal vaccines and in many cases those variants were more dangerous and harder to treat with antibiotics (e.g., see this study, this study, this study, this study, this study, this study, this study, this study, this study).
Does developing a population-wide vaccine immunity to a disease improve or worsen the disease’s consequences?
Two
of the best examples of this were the chickenpox vaccine and the
measles vaccine (two relatively benign diseases in the era preceding
vaccination due to a robust herd immunity).
If
you get chickenpox as a child, it is benign, but if you get it as an
adult, it can often give you a horrible (and sometimes recurrent) case
of shingles. The CDC eagerly expected rolling out the chickenpox vaccine
would decrease shingles, but the opposite instead happened
(so they, of course, suppressed the data). The researcher who conducted
those studies, with a good basis for doing so, theorized that this
happened because the reduction of chickenpox in the population prevented
people from having their immune response to it be periodically boosted
by natural exposure.
In the case of measles, if
there is no pre-existing immunity and poor living conditions (e.g.,
widespread vitamin A deficiency), the disease can be horrible (e.g. measles killed 10% of Native Americans it infected in one outbreak). In the past, infants received antibodies from their mother’s milk (the importance of breast feeding is discussed here),
which provided them sufficient protection to build up permanent natural
immunity once they were exposed to the virus. The population-wide herd
immunity we used to have does not exist now, and periodic measles
outbreaks still occur despite the majority of the population being
vaccinated. Because we lack that immunity, many are vulnerable to
measles, which is always addressed by vaccinating even more people for
the disease.
What this means is that when the
measles vaccine was introduced, it was not needed (as measles deaths had
virtually disappeared), but since it’s widespread adoption, it’s
essentially become “necessary” because herd immunity to the disease no
longer exists and there will hence be measles outbreaks once infected
individuals enter the community. Fortunately, despite around 1,500
measles cases happening since 2019, it has not led to any deaths (although there were quite a few hospitalizations).
Is there a benefit to developing the disease naturally that is prevented by vaccination?
One
of the lesser known facts about diseases is that childhood infections
are often critical for helping the immune system develop. In turn,
avoiding a (relatively) childhood infection can predispose one to a much
worse disease later in life. For example, a belief exists within Anthroposophic medicine
that the childhood infections train the immune system to fight cancer,
and research in turn supports this for some of the deadliest cancers:
•Not having a chickenpox infection increasing your risk of brain cancer later in life (e.g., see this study, this study, this study, and this study).
•Not having a mumps infection increasing your risk of ovarian cancer, one of the most deadly cancers for women (see this study, this study, this study).
Note: this preventative effect was also found for measles, rubella and chickenpox infections.
•Previous infections of influenza, measles, mumps or chickenpox were found to decrease one’s risk of malignant melanoma.
Note: another study found similar results.
Vaccinating While Infected
If you are already infected at the time you receive the vaccine, does this improve or worsen your response to the infection?
As I discussed in a recent article, there is a significant degree of evidence showing that receiving a vaccine while infected causes the existing infection to become much worse (e.g., it can spiral out of control). For example, the data that Merck submitted to the FDA showed that if you had a pre-existing HPV-16 or -18 infection, your risk of developing a cancerous lesion was increased by 44.6% following vaccination.
Likewise, we’ve seen many cases where a COVID-19 vaccination significantly worsened an existing COVID-19 infection, and many cases which suggested an influenza vaccine did the same for the flu.
Additionally, abundant historical evidence shows that vaccination also significantly worsened pre-existing typhoid, influenza, and polio infections.
Unfortunately, a pre-existing infection is never tested for before vaccination, which I suspect was because it was known that doing so would decrease vaccine sales.
Vaccine Side Effects
One of the important things to understand about toxins is that their side effects are distributed on a bell curve, which means that their side effects become increasingly rarer as they increase in severity. Although the severe reactions are the most noticeable (e.g., the rapid progression to lifelong autism or sudden infant death syndrome), less severe chronic complications are much more common, and in my opinion, create the greatest burden on society.
An explosion of chronic illness (particularly of neurological and autoimmune nature) in our society has paralleled the mass vaccination of society. This has been most apparent at three times in history: the period of the smallpox vaccines, after 1986 when Congress passed legislation to shield manufacturers from liability for producing dangerous vaccines (which led to a rapid increase in the number of childhood vaccinations and no motivation to ensure their safety), and following the COVID-19 vaccines. In each case, we’ve tragically become acclimated to an increase in baseline levels of chronic illness which never existed in the past, and we have simply assumed that the current disease burden is normal, when in reality it is not.
Similarly, although the sudden deaths from the COVID-19 vaccine are tragic, many less severe but debilitating or disabling reactions are much more common.
As
the effects of mass vaccination are so broad, it is often difficult to
even begin scratching the surface of what’s happened or to accurately
quantify them. Sadly, the things that could most accurately assess this
(randomized trials comparing the vaccinated to unvaccinated or access to
databases that have the data) have been prohibited. Fortunately, some
data assessing this does exist, and for a wide range of common
conditions, those vaccinated are 3 to 50 times as likely to develop
them.
Note: I compiled the existing data showing the full extent of the harms of the vaccination program here. It is profoundly disturbing.
How easy is it to recognize that these effects occurred?
Given how difficult it is to get doctors to acknowledge the most extreme reactions to a childhood vaccine, it should come as no surprise that the more subtle issues go mostly unrecognized or are dismissed (to the point that members of the societal orthodoxy commonly produce memes making fun of anti-vaxxers who blame their various health issues on vaccines).
One of the struggles I have experienced throughout my career in medicine is the fact that I can notice right away that a vaccine injury has occurred while sadly, most of my peers cannot. Most of the signs that scream out to me are rarely detected by my colleagues, and the symptoms either don’t register or they give some type of innocuous explanation for them (e.g., it’s just a behavioral thing that requires an SSRI to treat). Furthermore, if I try to point them out, all it accomplishes is undermining my credibility.
This has been particularly tragic to watch with COVID-19, as countless patients are all developing the same symptoms after vaccination, and yet most doctors ardently insist they have nothing to do with the vaccines. Fortunately, this does appear to be beginning to change, as the medical field’s eyes are opening up to the issue (in part because many healthcare workers have also been injured).
How consistent and safe is the vaccine’s manufacturing process?
Because
vaccine manufacturers are exempt from liability for unsafe products
they produce, many corners often end up getting cut with the production
process so more money can be made by the manufacturer (to this point
America’s facilities that make our vaccines have been plagued with production concerns such as potential contamination) the FDA has done almost nothing
to address. Additionally, since many vaccines are grown in cell
cultures, contamination from things already present in the cells (e.g.,
retroviruses) is inevitable, and some believe this is a key issue
concerning vaccines.
With the COVID-19 vaccines, it
has been demonstrated that much less due diligence was done with
producing the vaccines (likely due to Operation Warp Speed enabling this
malfeasance) and as a result, there is immense variation in what is present in each vaccine.
Presently, this is the best explanation I have found for why people
react so differently to various vaccines and why “hot lots” exist.
Note: production quality issues (e.g., hot lots) are a longstanding issue with vaccines and have caused numerous disasters reaching back over 100 years.
Does the vaccine priming your immune system to target one pathogen reduce its ability to respond to other pathogens or cancerous cells within the body?
Off-target immunity is a frequent but under-appreciated consequence of vaccination (discussed further here). As far as I know, the worst offender in this regard has been the COVID-19 vaccines, which have been linked to an explosion of cancers and unusual diseases typically only seen in immune-suppressed individuals.
Does the vaccine impair circulation and cause microstrokes in the body?
I believe that this is one of the primary mechanisms of harm done by vaccines, and frequently what must be focused on when treating these patients (e.g., we have seen miraculous results for individuals with COVID-19 vaccine injuries who we treated with simple methods for addressing their zeta potential). As this is a complex but critically important subject to understand, I put together an article explaining it here, alongside an article and how to treat it here.
Does the vaccine cause the immune system to attack the body and give rise to chronic illnesses?
All
vaccines work by provoking the immune system to go into overdrive to
attack the vaccine antigen that is present. The downside to this is that
it typically also causes the immune system to attack other proteins in
the vicinity (e.g., a mice study
showed that mice develop allergies to pollen that is in the air at the
time of their vaccination). Autoimmunity is especially likely to happen
if the vaccine shares antigen sequences with human tissue (homologies)
and contains a very strong adjuvant (the vaccine component that
stimulates the immune system). Before the COVID-19 vaccines (which have a
remarkable number of homologies with human tissue), Gardasil (the HPV
vaccine) was the greatest offender here as it had to use a very strong
adjuvant and had homologies to human tissue.
Note: the link between vaccines and autoimmunity is discussed in more detail here.
If a vaccine causes negative reactions, does the risk increase if multiple vaccines are given concurrently?
Everything I have seen has shown that the more vaccines that are given (especially if they are received at the same time), the more likely people are to develop a severe reaction to the vaccine. This, for example, is why Sudden Infant Death Syndrome has been correlated to receiving multiple vaccines simultaneously, why many parents have observed their child developing autism after multiple vaccinations, and why some doctors advocate for not following the CDC schedule and spacing out the required vaccinations.
Similarly, if the same vaccine is provided multiple times (especially if it has tissue homology) each successive time it is given, it is more likely to create an autoimmune condition. Although I have seen this with other vaccines, this effect has been by far the most dramatic with the COVID-19 vaccines because their risk of a severe adverse event increases significantly with each successive vaccination.
Although increased autoimmune priming likely plays a role, I also believe the cumulative toxicity with vaccines is in part due to them successively impairing the zeta potential of the body, which creates catastrophic consequences once a critical threshold is passed (e.g., microclots and strokes). Analogously, I often see the worst responses to vaccines in individuals who already have an impaired zeta potential and cannot tolerate the additional reduction created by one more vaccine.
Unfortunately, since vaccines are considered “safe and effective” their potential harms are never considered. This is why individuals who try to propose very simple measures that could greatly mitigate the harm of the vaccination schedule (like spacing out vaccines) are relentlessly attacked under the justification that “they are not following CDC guidelines” and thus creating vaccine hesitancy.
If the vaccines cause negative reactions, who is the most susceptible to them?
There is a huge variation in responses to vaccines. Typically, individuals who have had a bad reaction to a vaccine are more likely to have bad reactions in the future, and there are a variety of other signs that predict the likelihood of a bad reaction to vaccines (e.g., previous adverse reactions, pre-existing autoimmune conditions, poor physiologic zeta potential, genetic metabolic defects, having previously had the infection the vaccine is for).
Unfortunately, since vaccines are considered 100% safe, virtually nothing qualifies as an exemption to them. To highlight the absurdity of it, I had a friend who had a documented anaphylactic reaction to the Moderna vaccine which they needed to go to the ER for, and was simply told that they should go get a different brand of the COVID vaccine. I have also heard of a case where someone was hospitalized in a California ICU for a vaccine reaction and could not find a doctor in the state who was willing to write a medical exemption for their employer (as California is known for taking away the licenses of anyone who writes vaccine exemptions).
The Public Health Perspective
One of the largest issues with public health is that it does not see people as individuals, but instead uses theoretical constructs (that are often wrong) and applies them to the entire population. I believe that this is done because it is the most practical way for a centralized bureaucracy to affect the health of a large swath of people with whom it has no direct contact with.
This approach is a huge problem because many individuals behave differently from others (e.g., some derive no benefit from the intervention and some react poorly to the interventions). Unfortunately, for the centralized public health approach to work, the public’s diversity must be ignored, and dissent must be forcefully suppressed when members of the public complain.
Many issues in life I believe ultimately come down to people being lazy and taking the easy way out when addressing a complex problem. For example, in a recent series on SSRI antidepressants, one way the entire debacle could be summarized is that patients with mental health issues require a therapeutic relationship with a counselor who can help them navigate their issues, but this is far too time consuming for most doctors in practice.
Psychiatric medications offer an easy way out; you can just give the drug for the symptom, feel like you solved it, and not have to deal with the patient. Unfortunately, this often doesn’t work, and the medications make the patients worse. At this point, the choice to do one’s job properly or default to a lazy approach again comes up. The doctor can actively monitor the patient for adverse reactions to their drug and intervene before those effects are catastrophic, or gaslight the patient, tell the patient the drug works and just give them more of it or another drug. Most of the catastrophic events I’ve heard about from SSRI-injured patients happened because the doctors took a lazy approach addressing their patients issues.
Similarly with public health, if a contagious disease is present that the system believes needs to be addressed, there are two options:
•Adopt comprehensive public health measures to contain and mitigate the spread of the disease and encourage practices that increase the population's natural immunity.
•Create a vaccine for it, add it to the vaccine schedule, and mandate it so everyone takes it.
Since the second approach takes much less work, it’s a foregone conclusion that it will happen. Similarly, since the approach will inevitably fail to prevent many people from catching the disease, excuses will be made for why this happens that ultimately boils down to “not enough vaccines were given.”
Likewise, it's inevitable that injuries will occur from these campaigns (which often outweigh any benefit achieved by the vaccines). When this happens, the centralized public health administrators write off those injuries as “necessary collateral damage” for the greater good that the vaccine creates, and system-wide policies will be adopted to conceal those injuries and gaslight the injured.
Typically, once it becomes clear that the vaccine is not completely “safe and effective” the justification provided to the public is that the vaccines create “herd immunity” to the disease and that this benefit outweighs the negative consequences of the vaccine. Unfortunately, in most cases (for many of the reasons listed above) the vaccines do not create herd immunity and instead become a product the population needs to take indefinitely while the disease continues to persist.
Recently, I received an email from a Colorado reader which illustrates the absurdity of the current paradigm:

Note: for those interested in this subject, I discussed how vaccines consistently fail to prevent disease transmission here, and how we watched this unfold with the COVID-19 vaccines here. One of the things I find particularly unfair about this failure is that a common marketing tactic used to sell vaccines (particularly for pertussis and COVID-19) is by convincing everyone it’s not safe to be around an unvaccinated individual and hence create the peer pressure to vaccinate (e.g., grandparents periodically tell me they can’t see their grandchild because they refused to get a pertussis vaccine). Beyond the fact this is nonsensical (e.g., if the vaccine works it shouldn’t matter if other people are unvaccinated) as the above example (and what we saw throughout COVID-19) showed, it’s also patently false.
Which Vaccines Should Be Avoided?
For each vaccine, as we consider the risk of its disease, the efficacy of the vaccine, the effects of developing vaccine immunity within a population, the issues with vaccinating while infected, and vaccine side effects, it should become clear that this is an immensely complex question to answer. There are so many potential risks and benefits of different magnitudes that combining them into a weighted average borders on the impossible.
This helps to illustrate some of the major issues that arise when you provide an intervention with known harms as a preventative for a potential risk that may or may not happen (note: the same can also be said for many other toxic pharmaceuticals like statins).
My own belief is that if a therapy has known harm, the benefit for it needs to be concrete (e.g., all antibiotics are to some extent toxic, but most would agree that toxicity is outweighed if someone has a dangerous infection the antibiotic will treat). In the case of vaccination, there are a few vaccines that can be given therapeutically (BcG, rabies, and ones made from the patient’s own serum) to treat an existing issue, so a clear understanding can be reached about the relative risks and benefits of each, but that is not the case for virtually every other vaccine on the market.
Typically speaking, to analyze complex questions like this, we depend on large clinical trials. The problem with such trials is that since they are industry-funded, they always omit most of the adverse events that arise (e.g., they reclassify a severe event as something nebulous, they use a toxic placebo to mask the increase in adverse events seen amongst the vaccinated, they never evaluate for a variety of the common side effects or they only monitor subjects for a brief period of time, which is not long enough for most of the vaccine side effects to appear). Generally speaking, the only way to get around this issue is to assess the total number of people who die in each group (as there is no way to reclassify death), and when this metric is looked at in the trials for the worst vaccines (e.g., Gardasil or Pfizer’s COVID-19 vaccine) the total death rate is shown to be increased by vaccination.
The other option is to look at population statistics. Sadly, while these consistently show vaccines cause significant harm, public health officials tend to ignore this data.
When I approach this question, I use the following algorithm, where each item takes precedence over the ones after it.
1. Does the vaccine have an unusually high degree of toxicity?
2. Does the vaccine potentially provide an important benefit?
3. Does the vaccine have other reasons to make me concerned about its potential side effects?
4. Does the vaccine actually work?
5. Does the vaccine still work?
For example, let’s consider two of the currently recommended vaccines with the worst risk to benefit ratio
COVID-19
Although many tragic things have happened with the COVID-19 vaccines, the circumstances around them have also made it possible to shed light on the actual risks and benefits of vaccines in general, a topic that is typically far too obfuscated for anyone to make sense of. The clarity this time around is primarily because:
•The novel vaccines were rapidly rolled out to the entire population at the start of 2021. This makes it possible to compare numerous existing yearly trends before and after the deployment of the COVID-19 vaccines.
•A lot of people strongly objected to how the vaccines were pushed onto the population, and did a lot of work to prove that the risks from these vaccines greatly outweighed their benefits in almost every aspect that -was examined.
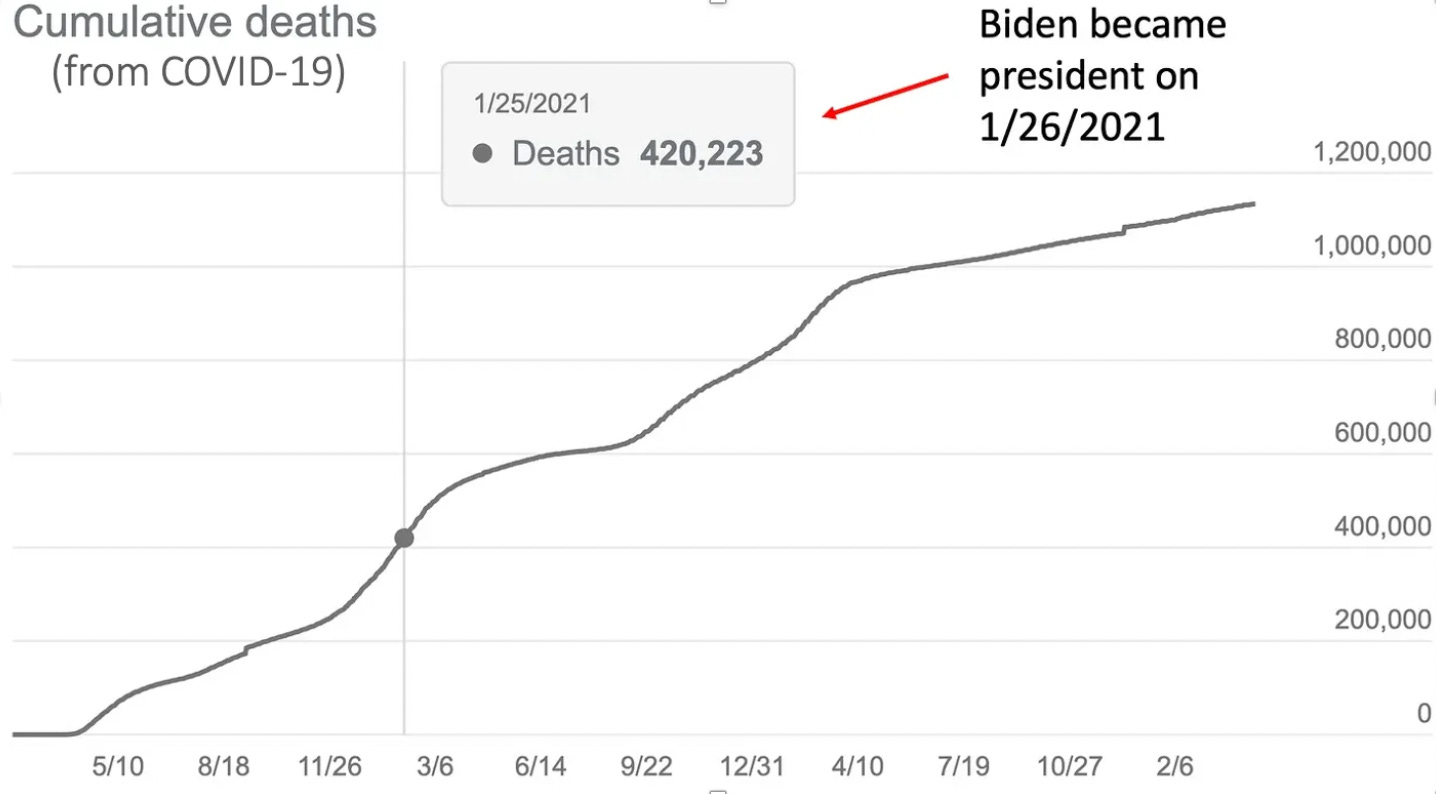
For example, many people are aware of this dataset (which like many others showed COVID-19 death rates increased after the vaccines hit the market, and now, years later, we still do not have herd immunity to the disease):
Likewise, severe injuries from the vaccine are common. Beyond personal experience or the experience of those directly connected to us, over a dozen polls have found that 47-57% of Americans think the vaccines aren't safe, 9-34% were injured by them (with 7% reporting major side effects) and 10-28% know someone the vaccines injured or killed.
The best assessment I’ve seen of the impact of these vaccines came from the report Ed Dowd’s team put together, which I must note was conservative in its estimate (because they didn’t want to claim harms they suspected were there but did not have the data to support):
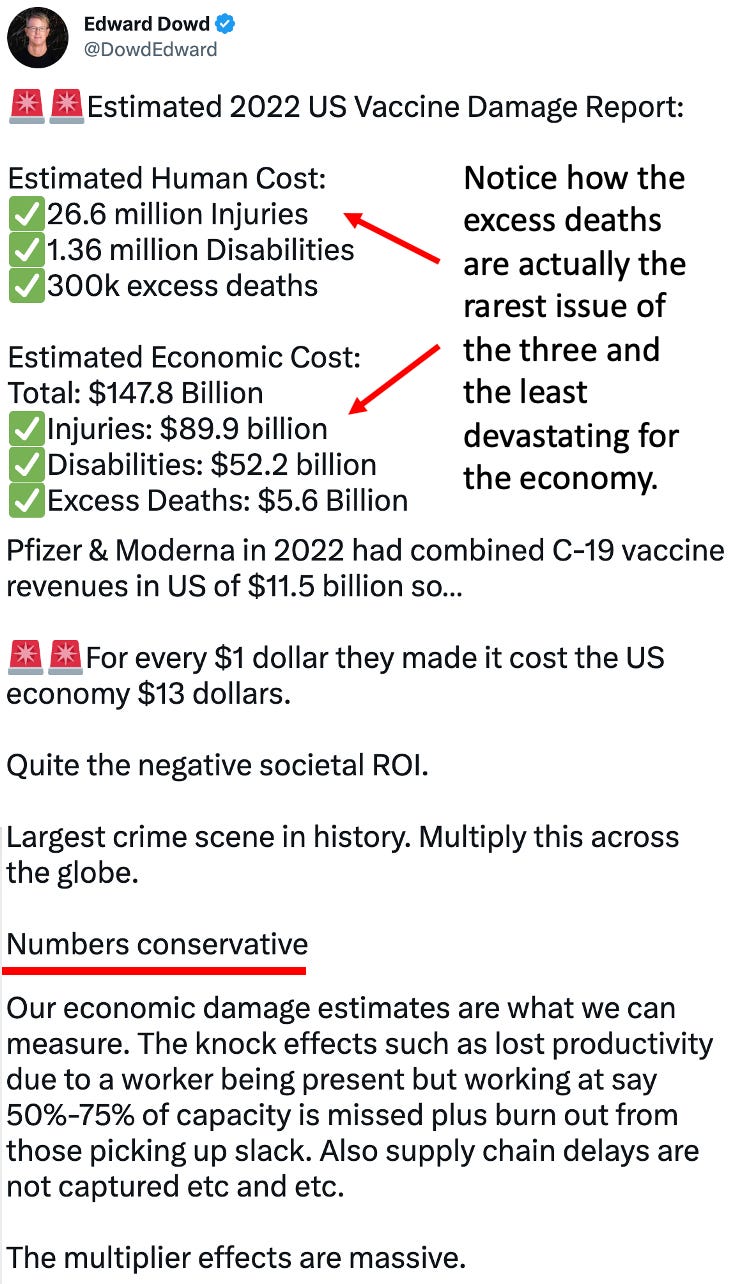
That’s insane and something almost no circumstance could justify (short of a deadly disease that had a real risk of making humanity go extinct).
Gardasil
In the case of the HPV vaccine, its benefit arises from “preventing cervical cancer.” Given that pap smears had mostly eliminated cervical cancer deaths, it's difficult to say if any real benefit arose from the vaccine. To illustrate:

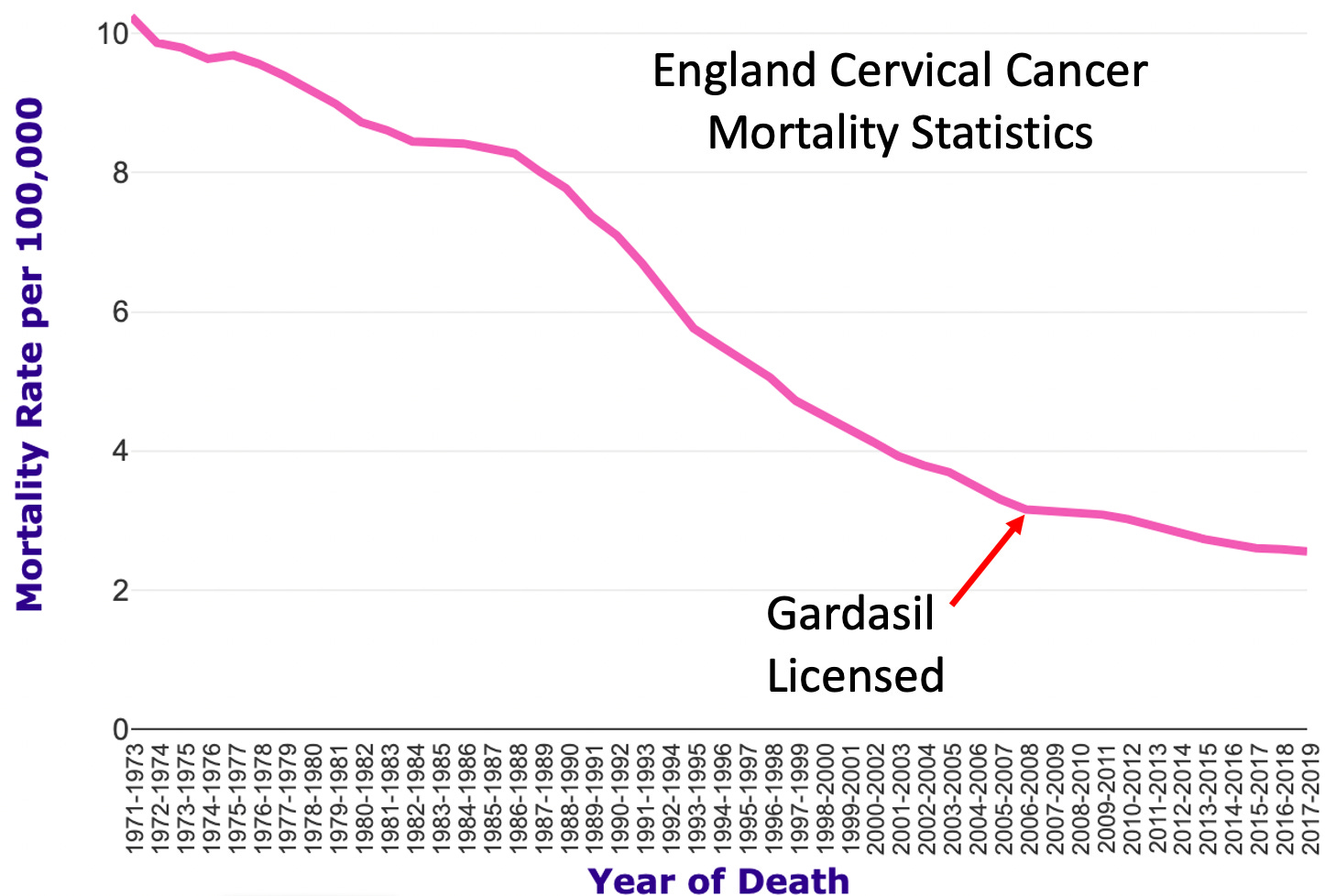
While
I have seen datasets (when stratified by age) showing Gardasil (and
other HPV vaccines) actually increased the cervical cancer death rate in
those vaccinated, I will give it the benefit of the doubt here. As the
graph shows, cervical cancer rates were already approaching 0 before
Gardasil, so it is difficult to say if any of the lives saved were due
to it (at this point I believe the cancer prevention attributed to
Gardasil is false).
Note: many other diseases whose decline was attributed to vaccination also actually had most of their decline occur prior to a vaccine being available.
However, assuming all lives were saved by Gardasil, in England, each year it has saved 6 lives per 100,000 (0.0006%) people, and in the United States, 2 lives per 100,000 (0.0006%) people. Conversely in the clinical trials, 133 per 100,000 (0.13%) participants died (in comparison, the average death rate at the time for those the same age as the trial participants was 43.7 per 100,000). This means, in the best case scenario for the vaccine, for 100,000 people you traded killing 89.3 of vaccine recipients early in life in return for saving 2 later in life.
Even though this is terrible, the greater issue is that in the original HPV clinical trial, between 2.3% to 49% of the individuals who received Gardasil developed a new autoimmune condition. We do not know exactly where in that range the total number of new autoimmune disorders was, as Merck classified many autoimmune disorders simply as “new medical conditions” (industry trials always reclassify something they don’t want to show up in the final trial with vague labels like this), but other investigations have concluded the 2.3% figure significantly underestimated the rate of new autoimmune conditions.
So, in return for saving 2 lives per 100,000 people while killing 89.3, you are also giving 2300 (and likely many more) a new life-altering autoimmune condition. All in all, I would not say this represents the best risk-to-benefit ratio. Unfortunately, because Gardasil is so profitable, nothing has been done about this despite numerous red flags being set off and many petitions being made to the FDA to address it. Sadly, as insane as that is, as the COVID-19 vaccines show, that’s not an anomaly.
Risks and Benefits of Other Vaccines
Note: as hundreds of vaccines exist, I am restricting my focus henceforth to those on the CDC schedule.
As I’ve shown in this article, it’s often quite clear it’s hard to justify taking a recommended vaccine. At the same time however, in many other cases it’s much less clear where the risk/benefit cutoff lies, particularly since the information we receive is greatly biased in favor of the vaccine and much of the research that should have been done to establish its benefit simply doesn’t exist.
Since the vaccine issue is quite polarized (most individuals in it either are opposed to all vaccines or strongly support all vaccines) I’ve tried to look past my own biases and objectively assess which vaccines have the strongest justification. I believe this is important both because that mindset allows you to reach people on both sides of the issue and because I believe making people avoid the worst vaccines (and spacing the remaining ones out) is something many would agree to and something that would greatly reduce the harm of our vaccination program.
In the final part of this article, as I have been researching this extensively over the last year, I will share my current thoughts on each of the vaccines on the CDC schedule:



Commentaires
Enregistrer un commentaire